The 5 Languages of Psychiatry: Speaking with Each Other, Listening to Each Other…
By: Gordon Harper MD, Associate Professor of Psychiatry, Harvard Medical School, United States.
There is a challenge in Psychiatry we don’t talk about: the five languages we use when we talk with each other and with patients.
These languages can be named and defined as follows:
- Descriptive: an objective listing of symptoms
- Categorical: the words used, as in the DSM or ICD 11, to name a pattern of symptoms, called a disorder
- Experience-near: ordinary language that captures the experience of the person
- Etiological: hypothesized origins (genetic, early life, current stressors and context; brain functioning)
- Developmental-recovery: placing each symptom in a process of growth, learning, and adaptation – where is the person on that path?
To illustrate these let’s apply them to one condition, borderline personality disorder:
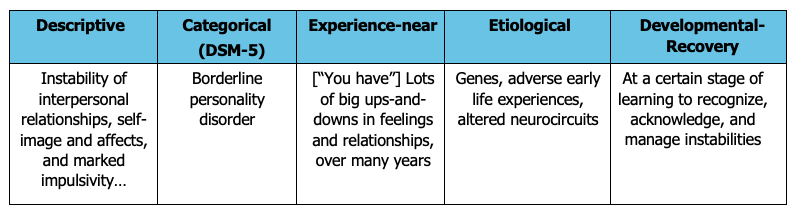
Figure 1: Category of Five Languages
Regarding any condition, we can ask:
- What words does the person use for their condition?
- What words has the person heard professionals use?
- How has the person felt about the words used?
- Do the words fit? How do the words make the person feel? Different? Sick? Ashamed? Hopeful? Understood? Respected?
These different ways of speaking differ from the perspectives of Psychiatry delineated by McHugh and Slavney: diseases, dimensions of personality, goal-directed behaviors, and life stories. Here we focus not on where our ideas come from, but on how we speak. We consider these different languages, acknowledge the confusion (and sometimes distress) that patients and family members feel in hearing these terms applied to themselves or their loved ones, and offer suggestions as to how we might do better.
How it Feels to Patients
People respond differently to getting a psychiatric diagnosis. For some, the diagnosis is clarifying and enhances personal dignity: “At last I felt it wasn’t a personal failing of mine, but a medical condition that anyone could have.” Diagnostic findings can strengthen this positive – and appreciated – redefinition of the problem.
At the other extreme, the diagnosis can feel like a confirmation of something “objective” but experience-distant. “I don’t want to be given another medical jargon term – I want someone to understand what it’s like for me.”
With patients be sure to ask, not just what diagnosis the patient may have been given in the past, but to ask as well, How did they understand that diagnosis, How did it fit or not with their experience, and How did they feel about it?
Feeling Understood
Key to how the patient feels about the diagnosis is how much he or she feels understood – feels that someone “gets it”. The importance in human development of feeling understood – or not – “Nobody understands me” - has not been reflected appropriately in the psychiatric literature – or the developmental literature in general. I have collected phrases that help patients feel understood – or not.
There are a few take-homes from this review.
One, do not assume that diagnostic statements, in language that works for us, will work for the patient. Be curious!
Second, review the statements that are affirming and validating, and contrast them with those that are the opposite. Receptivity, appreciation, validation – “I get it” – are most useful responses. Especially, avoid defensive statements, saying something like, “Well, there may be more than one way to see that,” as opposed to, “But really, what happened was…”
Third, shun the use of the pseudointerrogative “Why?” as in, “Why did you walk into my clean kitchen with your muddy boots on?” in which there is clearly a reproach hiding beneath the inquiry.
Fourth, frame information, wherever possible, in the terms of growth, learning, and healing, rather than as static conditions. Rather than, “Father died when he was four” try to frame that in terms of recovery: “Father died when he was four and family never talks about him – question of frozen grieving.” Or, rather than, “Got the diagnosis four months ago and won’t talk about it” try, “At an early stage of…”
Ways Forward
- Include this topic, of the usefulness of acknowledging the unacknowledged, in curricula.
- Collect stories that illustrate the power of the uncoordinated languages.
- Develop clinical exercises for students, featuring different languages and asking the student how to manage the differences.
Further Studies
- Does something like the Five Languages occur in other specialties?
- What about in settings with other languages? With other cultures? Apart from the U.S.?
- Does Intervention lead to better patient outcomes?
This article represents the view of its author(s) and does not necessarily represent the view of the IACAPAP's bureau or executive committee.