No Child Should Fall Between Systems: Building Kosovo’s pathway for adolescents with substance use and behavioural difficulties
By: Dr Lirim Isufi1 and Dr. Adelina Ahmeti Pronaj2
1 Child and Adolescent Mental Health, Kosovo
2 Assistant Professor, Child and Adolescent Mental Health, Kosovo
Key Message
Adolescents with substance use and behavioral difficulties should not have to move from school to psychiatry, from family to social services, and from crisis to justice without a clear pathway of care. Kosovo does not need another isolated response. It needs one coordinated adolescent pathway.
This article makes a practical argument for a coordinated, developmentally appropriate pathway for adolescents whose difficulties sit between mental health, substance use, family strain, school disengagement and social risk. The argument is written for a global audience, but it is grounded in the service realities of Kosovo. Since adolescent substance use is sensitive and often stigmatized, available survey figures should be treated as conservative indicators, not as the full burden.
Data highlights
- 4,531: students included in Kosovo's first HBSC survey
- 4.7%: reported being active smokers
- 10%: reported alcohol use
- 1.5%: reported cannabis use in the last 30 days
- 77%: of youth surveyed were concerned about coping with stress
- 56%: of respondents aged 12-16 said school grades were a source of stress
Sources: HBSC in Kosovo (UNFPA/UNICEF/Ministry of Health/Ministry of Education); UNICEF Situation Analysis of Children and Adolescents in Kosovo. Self-reported figures may underestimate true use because of stigma, confidentiality concerns and school-based sampling limits.
Introduction
In practice, the adolescents who worry clinicians and families most are rarely defined by one symptom. A young person may be using cannabis, missing school, staying out late, becoming aggressive at home or drifting towards the street. What looks like “bad behavior” is often a more complicated mix of distress, impulsivity, family strain, school disengagement and unmet mental health need.
These young people can fall between systems. A school-only response may not be enough. A brief outpatient appointment may not hold the complexity. Adult addiction services are usually not designed for them, and leaving the burden entirely with the family is unsafe and unfair. The result is familiar: crisis, blame, fragmented action and delay.
Kosovo faces this gap clearly. It is not starting from zero: there are already important pieces of care across health, education, social welfare and justice. What remains limited is a specialized and coordinated rehabilitation route for adolescents whose substance use appears together with behavioral, emotional, family and social difficulties.
Why this matters
Adolescence is a developmental window in which reward seeking is heightened, while the systems responsible for planning, inhibition and longer-term judgement are still maturing. Substance use during this period is therefore more than a behavior problem. It can become a developmental and psychosocial risk, especially when it is combined with trauma, peer risk, school exclusion or family breakdown.
The World Health Organization estimates that one in seven adolescents aged 10-19 lives with a mental disorder globally [1]. In Kosovo's first Health Behavior in School-aged Children survey, which included 4,531 students aged 11, 13 and 15, 4.7% reported active smoking, 10% reported alcohol use and 1.5% reported cannabis use in the last 30 days [3]. These figures do not suggest a population-wide substance-use crisis, but they do justify early, organized intervention, particularly when substance use appears alongside violence, school exclusion, trauma or family breakdown.
These figures also need caution. Because adolescent substance use is stigmatized and usually measured through self-report, prevalence estimates may be affected by social desirability, fear of consequences and confidentiality concerns [6,7]. In Kosovo, disclosure may also be shaped by family reputation, school discipline and legal fears. The observed percentages are therefore best read as conservative indicators. The true burden may be higher, especially among adolescents outside school or already moving through health, welfare, or justice systems.
A recent UNICEF situation analysis adds a parallel concern: 77% of young people surveyed in 2021 said they were worried about coping with stress, and 56% of respondents aged 12-16 in a 2024 survey said worries about school grades were a source of stress and anxiety [4]. The same analysis notes that services for children and adolescents are not adequate to meet demand, and that school psychologists are often overburdened [4]. The European Union Drugs Agency likewise notes that Kosovo's national drug monitoring system is still developing, with reporting organized through the National Drug Observatory [5].
Figure 1. Fragmented sectors and a coordinated pathway
Figure 1: Fragmented sectors only become clinically useful when they are connected by one adolescent rehabilitation pathway.
The gap is not only clinical; it is structural
The adolescents most in need rarely arrive saying, “I have a substance use disorder.” They arrive through events: school exclusion, police contact, self-harm, intoxication, family exhaustion or repeated refusal to attend appointments. If each sector responds separately, the young person receives pieces of care but not a coherent plan.
A punitive response may temporarily stop one behavior without addressing the underlying pattern. A purely medical response may miss the family and school context. A purely psychological response may fail if daily substance use, social risk or acute safety concerns remain unchanged. What is missing is not goodwill. It is coordination.
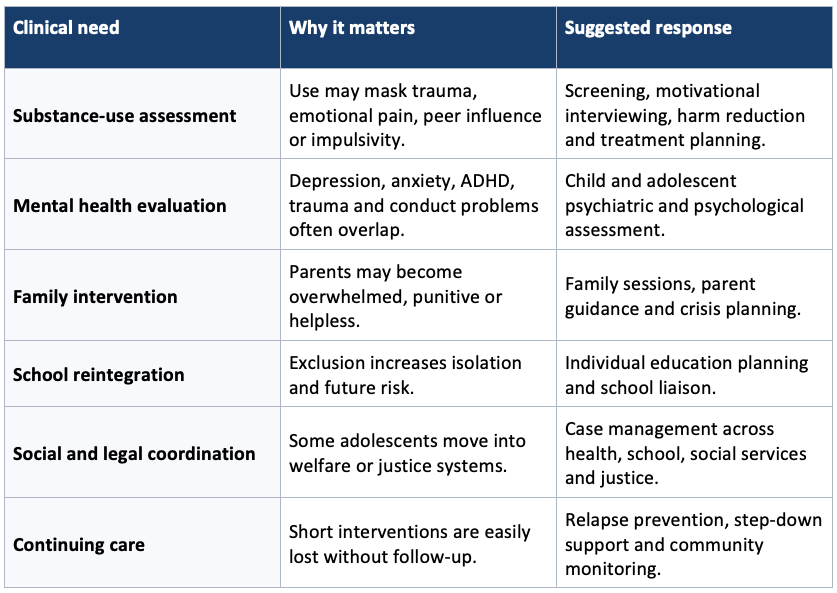
Table 1. Core elements of an integrated adolescent rehabilitation pathway
What Kosovo could build
A useful response does not need to begin with a large residential institution. For Kosovo, a realistic sequence could start with a specialized outpatient pathway, develop an intensive day program for adolescents who need closer support, and later add crisis beds and structured follow-up for a smaller group of high-risk cases. The key issue is not the building. It is the sequence, referral criteria and continuity of care.
The pathway should connect child and adolescent mental health, pediatrics, schools, social workers, police, courts and community organizations. It should include staff training, supervision and culturally adapted intervention tools. In a small health system, the strength of the model will come less from institutional size and more from disciplined coordination.

Figure 2. A feasible phased model for implementation.
A call for collaboration
Kosovo can build a careful, humane, and useful model. The need is not only for more services; it is for a model that holds the adolescent across systems. International collaboration could support this through technical advice, staff development, service design and exchange with established programs in adolescent mental health, addiction, education and social protection.
Kosovo can also contribute to the wider field. In smaller systems, fragmentation is easier to see. When a child is shared across five sectors but truly held by none of them, the problem becomes visible. This is not only a Kosovan problem; it is a global one.
The clinical question should not be “Whose problem is this child?”
It should be: “What pathway does this child need, and who will hold it with the family?”
Conflict of Interest Disclosure
The authors declare no conflict of interest related to this submission.
References
- World Health Organization. Mental health of adolescents [Internet]. Geneva: WHO; 2025 [cited 2026 May 8]. Available from: https://www.who.int/news-room/fact-sheets/detail/adolescent-mental-health
- National Institute on Drug Abuse. Principles of adolescent substance use disorder treatment: a research-based guide. Bethesda (MD): National Institute on Drug Abuse; 2014.
- United Nations Population Fund Kosovo, Ministry of Health, Ministry of Education, Science and Technology, UNICEF Office in Kosovo. Health Behaviour in School-aged Children in Kosovo: Final report. Pristina: UNFPA; 2014.
- United Nations Children’s Fund Kosovo. Situation analysis of children and adolescents in Kosovo. Pristina: UNICEF; 2025.
- European Union Drugs Agency. Kosovo: data sheet [Internet]. Lisbon: EUDA; 2024 [updated 2026 Apr 24; cited 2026 May 8]. Available from: https://www.euda.europa.eu/publications/2024/ipa-data-sheets/kosovo_da
- Brener ND, Billy JOG, Grady WR. Assessment of factors affecting the validity of self-reported health-risk behavior among adolescents: evidence from the scientific literature. J Adolesc Health. 2003;33(6):436-457.
- Khalil P, Esmaeili Nadimi A, Baradaran HR, Janani L, Rahmani A, et al. Validity of self-reported substance use: research setting versus primary health care setting. Subst Abuse Treat Prev Policy. 2021;16:86.
This article represents the view of its author(s) and does not necessarily represent the view of the IACAPAP's bureau or executive committee.